Diphtheria
Farah Haider
Corynebacterium diphtheria
Corynebacterium diphtheria is anaerobic, Gram-positive, non-motile, non-spore-forming, non-capsulated, toxin-producing, pleomorphic coccobacillus which is usually club-shaped. C. diphtheria has four biotypes, namely, gravis, mitis, intermedius, and belfanti. C. mitis is responsible for mild, C. intermedius is an intermediate form, and C. gravis is a more severe form of the disease.

A Little History
A German bacteriologist named Friedrich Loeffler (1852-1915) was the first to grow Corynebacterium diphtheriae. Loeffler utilized a series of principles known as Koch's postulates to prove that Corynebacterium diphtheriae was the cause of diphtheria. Later that year, in 1884, Loeffler discovered that C. diphtheriae generates a toxin. This was the first time a bacterial exotoxin was identified.
Diphtheria in the Lab
Diagnosis of diphtheria is confirmed by culture of the organism from the specimen and by demonstrating toxin production using an immunoprecipitation reaction. This is known as the Elek Test which is used to determine whether the culture is C. diphtheriae. C. diphtheriae can be viewed using electron microscopy which allows for finer details to be seen by researchers.
Symptoms and Severity

C. diphtheriae is spread from person to person by close respiratory contact and direct touch. C. diphtheriae has an incubation period of two to five days. Diphtheria symptoms include a thick grey-white coating at the back of your throat, a fever of 38 degrees Celsius or higher, a sore throat, headaches, inflamed glands in your neck, and trouble breathing and swallowing. When C. diphtheriae colonizes the upper respiratory tract, it secretes a toxin that injures and ultimately kills cells. Over the throat, waste materials and proteins combine to create a thick gray layer known as a pseudomembrane. The pseudomembrane adheres to tissues and may prevent breathing. Meanwhile, the poison might enter the heart, muscle, kidneys, liver, and other organs. DT (Diphtheriae Toxin) helps other bacteria to evade the immune response hence causing more severity in cases. In case of C. diphtheriae, it is known that macrophages show a delay of phagolysosome formation when being infected with different C. diphtheriae strains. However the mechanism is poorly understood.
.
Treatment Options
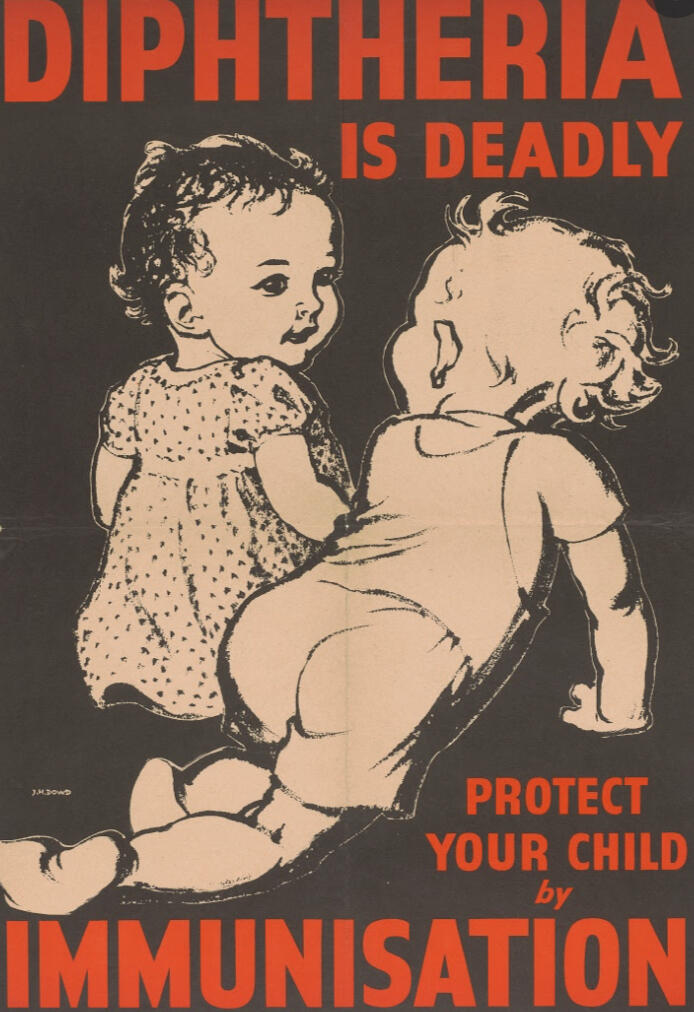
Diphtheria antitoxin is used to prevent the bacteria's toxin from causing harm to the host. This therapy is critical for diphtheria respiratory infections, although it is rarely utilized for diphtheria skin infections. Antibiotics are used to destroy and eliminate germs. Erythromycin and penicillin are the traditionally recommended antibiotics of choice for treating confirmed cases of early-stage diphtheria, though there are several different classes of antibiotics available to treat the infection. This is crucial for diphtheria infections in the respiratory system as well as those on the skin. Diphtheria patients are typically no longer able to infect others 48 hours after starting antibiotics. However, it is critical to finish the entire course of antibiotics to ensure that the germs are entirely eliminated from the body.
Today, four types of vaccinations are used to prevent diphtheria, all of which also protect against other diseases: DT vaccinations for diphtheria and tetanus vaccines, DTaP (diphtheria, tetanus, and pertussis) vaccinations, tetanus and diphtheria (Td) vaccines, and tetanus, diphtheria, and pertussis (Tdap). Babies and children under the age of seven are given DTaP or DT, while older children and adults are given Tdap and Td.
Diphtheria in the World and in the Future

The number of diphtheria cases reported globally has been increasing gradually. In 2018, there were 16,651 reported cases, more than double the yearly average for 1996-2017 (8,105 cases).
In recent studies, researchers discovered variations resistant to six of these classes in isolates from the 2010s, which was more than in any other decade. Because the diphtheria vaccination is meant to neutralize the toxin, any genetic variations that affect the structure of the toxin may have an influence on how successful the vaccine is. While our data does not indicate that the presently utilized vaccination is useless, the fact that we are witnessing a rising diversity of tox variants implies that the vaccine, as well as therapies that target the toxin, the vaccines must be improved.
© Untitled. All rights reserved.
Sources
https://www.cdc.gov/diphtheria/about/diagnosis-treatment.html
https://www.cdc.gov/vaccines/vpd/diphtheria/index.html
Chaudhary A, Pandey S. Corynebacterium Diphtheriae. [Updated 2020 Sep 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559015/
Murphy JR. Corynebacterium Diphtheriae. In: Baron S, editor. Medical Microbiology. 4th edition. Galveston (TX): University of Texas Medical Branch at Galveston; 1996. Chapter 32. Available from: https://www.ncbi.nlm.nih.gov/books/NBK7971/
Will R C, et al. Spatiotemporal persistence of multiple, diverse clades and toxins of Corynebacterium diphtheriae. Nat Commun 12, 1500 (2021). https://doi.org/10.1038/s41467-021-21870-5